
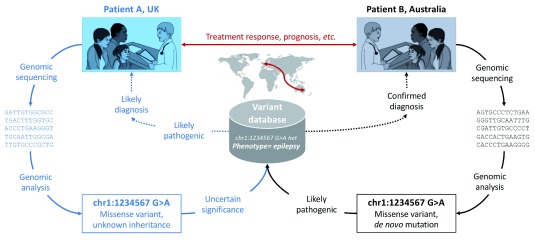
Sharing de-identified genetic variant data is necessary for the observe of genomic medicine and is demonstrably helpful to victims. Robust genetic diagnoses that inform medical administration cannot be made exactly regardless of genetic examine outcomes from completely different victims, along with inhabitants controls.
Errors on this course of might find yourself in delayed, missed or defective diagnoses, leading to inappropriate or missed medical interventions for the affected particular person and their family. The benefits of sharing explicit particular person genetic variants, and the harms of not sharing them, are fairly a few and well-established.
Databases and mechanisms exist already to facilitate deposition and sharing of pseudonomised genetic variants, nonetheless readability and transparency spherical most interesting observe is required to encourage widespread use, cease inconsistencies between completely completely different communities, maximise explicit particular person privateness and assure public perception.
We as a result of this truth advocate that widespread sharing of a small number of explicit particular person genetic variants associated to restricted scientific information should develop to be customary observe in genomic medicine. Information robustly linking genetic variants with explicit circumstances is essential natural information, not non-public information, and as a result of this truth should not require consent to share.
For additional case-level component about explicit particular person victims or further intensive genomic information, which is often necessary for scientific interpretation, it could be further acceptable to utilize a controlled-access model for data sharing, with the ultimate phrase function of setting up as a lot information as open and de-identified as doable with acceptable consent.
Clinical choices and outcomes of victims with Shwachman-Diamond syndrome and myelodysplastic syndrome or acute myeloid leukaemia: a multicentre, retrospective, cohort analysis.
Data to inform surveillance and remedy for leukaemia predisposition syndromes are scarce and proposals are largely primarily based totally on educated opinion.
This analysis aimed to analysis the scientific choices and outcomes of victims with myelodysplastic syndrome or acute myeloid leukaemia and Shwachman-Diamond syndrome, an inherited bone marrow failure dysfunction with extreme risk of making myeloid malignancies.
We did a multicentre, retrospective, cohort analysis in collaboration with the North American Shwachman-Diamond Syndrome Registry. We reviewed affected particular person medical info from 17 centres inside the USA and Canada.
Patients with a genetic (biallelic mutations inside the SBDS gene) or scientific evaluation (cytopenias and pancreatic dysfunction) of Shwachman-Diamond syndrome who developed myelodysplastic syndrome or acute myeloid leukaemia had been eligible with out additional restriction.
Medical info had been reviewed between March 1, 2001, and Oct 5, 2017. Masked central evaluation of bone marrow pathology was carried out if accessible to confirm leukaemia or myelodysplastic syndrome evaluation. We describe the scientific choices and common survival of these victims.
We initially acknowledged 37 victims with Shwachman-Diamond syndrome and myelodysplastic syndrome or acute myeloid leukaemia. 27 victims had samples accessible for central pathology evaluation and had been reclassified accordingly (central evaluation concurred with native in 15 [56%] situations), 10 had no samples accessible and had been categorized primarily based totally on the native evaluation data, and 1 affected particular person was excluded at this stage as not eligible. 36 victims had been included inside the analysis, of whom 10 (28%) initially launched with acute myeloid leukaemia and 26 (72%) initially launched with myelodysplastic syndrome.
With a median follow-up of 4·9 years (IQR 3·9-8·4), median common survival for victims with myelodysplastic syndrome was 7·7 years (95% CI 0·8-not reached) and 0·99 years (95% CI 0·2-2·4) for victims with acute myeloid leukaemia. Overall survival at Three years was 11% (95% CI 1-39) for victims with leukaemia and 51% (29-68) for victims with myelodysplastic syndrome.